Normal body temperature guide
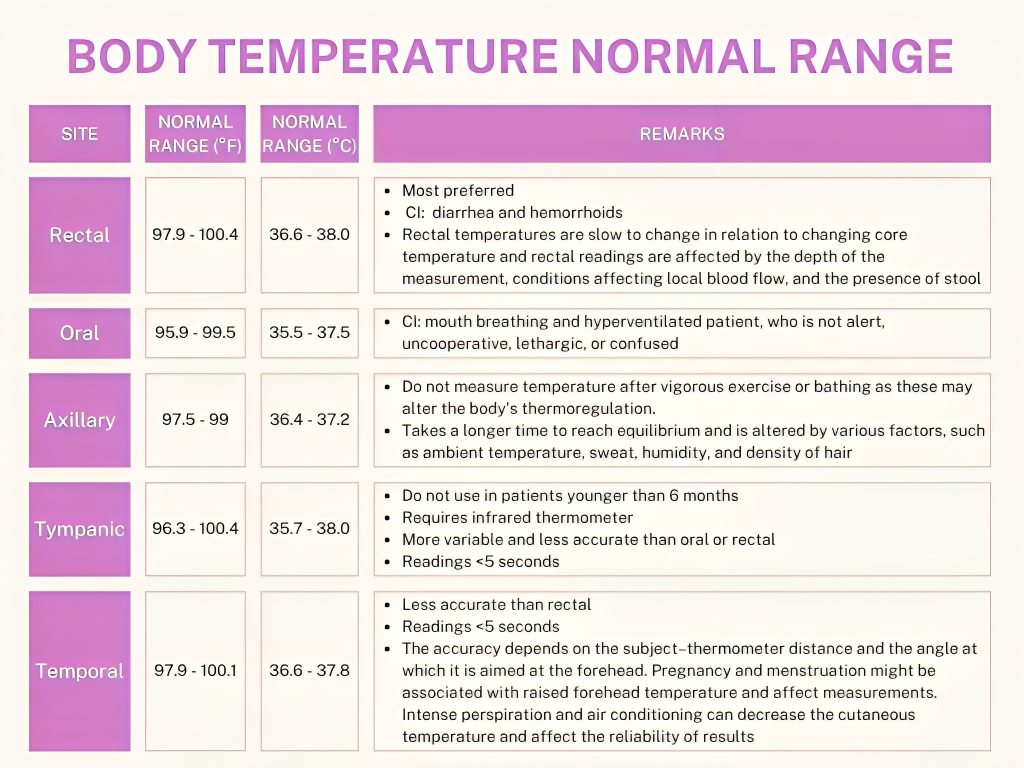
Know Proper Technique Of Temperature Measurement!!
Copyright © 2025 NEPHA. All rights reserved.